
The First Domino: How Losing Rural Birthing Services Affects More Than Births in Vermont
Rural healthcare systems across the United States are under increasing strain, and Vermont is already experiencing the effects. Hospital service reductions, provider shortages, and the growing number of maternity care deserts have contributed to longer travel times and reduced access to care, particularly in rural areas.¹,⁸ This is especially significant in Vermont, where more than 65% of residents live in rural communities.¹ One of the clearest—and often overlooked—indicators of these systemic pressures is the loss of rural birthing services.
These closures are not isolated events. Rather, they reflect a broader pattern in which demographic shifts, financial pressures, and healthcare infrastructure challenges interact. The loss of rural obstetric services is both a consequence of these forces and a contributor to further community decline—a “first domino” in a cascade of impacts affecting population stability, workforce sustainability, and local institutions.
I am a Master of Public Health student at the University of Vermont and have spent much of my life in New England, including in rural Maine and Vermont. Through both personal experience and academic training, I have observed how limited healthcare access shapes the daily realities of rural families. These challenges are not unique to any one state; they are part of a broader structural issue affecting rural communities across the country.
Vermont’s population trends provide important context. The state has experienced slow population growth in recent years, with a small decline observed in the most recent year of available data (2025).² At the same time, the population is aging, with nearly 42% of residents over the age of 50.² An older population contributes to lower birth rates and increased demand for healthcare services, while also reducing the size of the available healthcare workforce.
As shown in Figure 1, Vermont’s population skews older, with a higher proportion of residents in older age groups compared to younger cohorts.
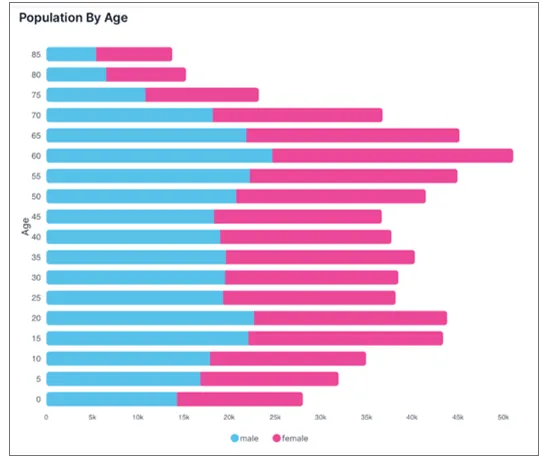
Figure 1. Age distribution of Vermont’s population, illustrating a higher proportion of older residents relative to younger age groups. An aging population is associated with declining birth rates and increased healthcare demand. Source: World Population Review (2024).²
Changes in migration patterns have also played a role. During the COVID-19 pandemic, Vermont saw an influx of residents relocating from metropolitan areas. However, more recent trends suggest that some of these individuals are leaving or reconsidering long-term residency.⁴ These shifts contribute to an already complex demographic landscape that affects both healthcare demand and service viability.
An aging population and declining birth rates are closely linked to the sustainability of maternity services. When fewer births occur in a given region, hospitals face challenges maintaining obstetric services due to the high fixed costs required to provide care. As Emily Sheffield, MPH, of the University of Minnesota Rural Health Research Center explains, “Providing birth care in a hospital has a lot of high fixed costs associated with it, including specialized clinical personnel and equipment that must be available 24/7. When birth volumes are low, hospitals may not generate enough revenue to cover those costs.”
In this context, the closure of labor and delivery units becomes more understandable. For example, Copley Hospital in Morrisville, Vermont, recently announced plans to close its labor and delivery unit amid broader financial pressures within the state’s healthcare system.³ These decisions are rarely made lightly; rather, they reflect the difficult reality that hospitals must balance community needs with financial sustainability.
The loss of local maternity services has immediate and tangible impacts. Pregnant individuals may need to travel longer distances to access care, which can create barriers to both routine prenatal visits and delivery.⁸ Longer travel times can also increase strain on neighboring hospitals, potentially affecting capacity and timely access to care. More broadly, reduced access to obstetric services can disrupt continuity of care and exacerbate existing disparities in healthcare access.
Beyond healthcare, these closures can influence broader community dynamics. Access to maternity services may influence where individuals and families choose to live. When essential services become less accessible, some families may opt to relocate to areas with more comprehensive healthcare infrastructure. Over time, this can contribute to population decline in rural areas, particularly among younger families.
Healthcare system changes also have economic implications. Hospitals are often major employers in rural communities, and the loss of services can result in job reductions and decreased economic activity. At the same time, broader trends in rural healthcare—including consolidation of practices and changes in provider employment structures—may affect how care is delivered and accessed at the local level.⁵
The effects extend even further, reaching community institutions such as schools. Declining birth rates and population shifts can lead to reduced school enrollment. In Burlington, for example, K–12 enrollment has decreased significantly over the past two decades, reflecting broader demographic trends.⁶ Schools serve as important anchors in many communities, and declining enrollment can place additional strain on already limited resources.
Healthcare access also directly affects students’ well-being and educational outcomes. Elizabeth Parris, BSN, RN, NCSN, a school nurse in the Winooski School District, describes these challenges directly: “Students were missing significant amounts of school for medical appointments that could have taken place after school hours. At the same time, some students were truly ill and unable to access the care they needed, which in turn affected their readiness to learn.” These challenges highlight how gaps in healthcare access can ripple into other aspects of community life.
Many rural hospitals operate with narrow financial margins. Vermont’s healthcare system is under significant financial pressure, and hospitals must navigate low patient volumes, high fixed costs, and limited reimbursement structures when making decisions about service offerings.³
Despite these challenges, efforts are underway to strengthen rural healthcare systems. Programs such as the Vermont Area Health Education Centers (VT AHEC) are working to build a pipeline of healthcare professionals by introducing students to careers in medicine and supporting training opportunities in rural settings.⁷ Community-based innovations, such as school-based health centers, are also helping to reduce barriers by bringing services directly to where people are.
These initiatives demonstrate that solutions are possible. However, without sustained investment and policy support, many rural communities will continue to face difficult tradeoffs in maintaining essential healthcare services.
The loss of rural birthing services is not solely a healthcare issue—it is a reflection of broader structural challenges facing rural communities. Addressing these challenges requires a comprehensive approach that considers not only healthcare delivery, but also demographic trends, workforce development, and community sustainability.
Protecting access to maternity care in rural areas is ultimately about more than ensuring safe deliveries. It is about supporting families, sustaining communities, and preserving the long-term vitality and future of Vermont itself.
References
- United States Census Bureau. 2020 Census: Rural America. Accessed April 2026. https://www.census.gov
- World Population Review. Vermont Population 2024. Accessed April 2026. https://worldpopulationreview.com/states/vermont
- Krupp L. State backs rural birthing center closure and warns of more “difficult decisions.” Vermont Public. 2025.
- Labare A. The rural health gap is growing: How Vermont is pushing back against a growing crisis. Northern Vermont AHEC. 2025.
- Physicians Advocacy Institute. Rural Physician Employment and Acquisition Trends: 2019–2024.
- Novak A. Vermont’s school enrollment is dropping at an alarming rate. Seven Days. 2026.
- Dougherty M, Petenko E. Where migrating Vermonters are going—and why. VTDigger. 2019.
March of Dimes. Nowhere to Go: Maternity Care Deserts Across the US. 2022.